Shoulder arthritis
What is osteoarthritis?
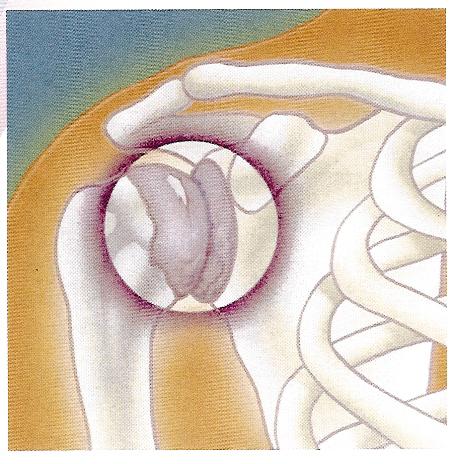
Osteoarthritis is a disease where the smooth articular cartilage coating the ends of the bone in a joint becomes damaged or worn away, exposing the underlying bone. The exposed bone then becomes diseased and deformed causing inflammation and severe pain. Arthritis occurs most commonly in the weight-bearing joints (knee, hip) that suffer the heaviest wear and tear; however it is also seen in the glenohumeral joint (where the ball at the top of the humerus fits into the glenoid socket) and the acromioclavicular (AC) joint of the shoulder. As it is a degenerative disease, it is most commonly seen in older patients (50 years plus).
What causes it?
Shoulder arthritis commonly occurs in patients who have had a previous shoulder injury (often many years before) which although it has healed has caused degeneration to the articular cartilage.
In the case of the AC joint, although it does not have to move very much, it is constantly under stress when your raise your arm above your head, and so arthritis is also seen in patients who have repeatedly lifted heavy weights overhead.
Rheumatoid conditions may also cause osteoarthritis.
How does it feel?
If you have arthritis your shoulder will be painful, stiff and your arm will feel heavy.
With glenohumeral arthritis, the pain may spread down your arm to your elbow, and you may feel a scraping sensation when you move your arm.
In AC joint arthritis, the pain increases if you bring your arm across your chest, and may spread from the shoulder to your chest and neck. There may be a bump over the joint, and your shoulder may make a scraping noise when you move it.
Diagnosis
After reviewing your medical history your doctor will make a physical examination of the shoulder to check your range of movement and to see which movements cause pain. He will also ask for X-rays to see if there are signs of arthritic degeneration – there will be a narrowing of the joint and possibly the formation of bone spurs (spikes or bumps of bone).
Treatment – conservative
Your doctor will initially prescribe rest, anti-inflammatory pain killers, and sometimes cortisone and/or hyaluronic acid injections. Physiotherapy treatments can be helpful for maintaining the range of movement and rebuilding the shoulder muscles.
Treatment – surgical
Glenohumeral arthritis
– Arthroscopic Debridement: this is performed in minor cases of arthritis, and is aimed at preventing or delaying further progression of the disease. Through two small incisions, and with the aid of an arthroscope (fibre-optic camera), the surgeon will clean up the joint, trimming any rough edges of cartilage, and removing loose particles of tissue.
– Bone Marrow Stimulation Procedures: abrasion arthroplasty and arthroscopic microfracture are two procedures that are performed to stimulate the bone marrow, making it form scar tissue or ‘fibrocartilage’, which replaces the damaged articular cartilage:
- Abrasion Arthroplasty – when the cartilage has worn away and bone rubs on bone, the bone-surface becomes hard and shiny. During arthroscopy, the surgeon can use a special instrument known as a burr to scrape off the hard, polished bone tissue from the surface of the joint. The scraping action causes a healing response in the bone, with new blood vessels entering the area, bringing stem cells, and causing the formation of fibrocartilage. The fibrocartilage that forms may not remove all the symptoms of pain in the shoulder, and therefore this may be only a temporary solution.
- Arthroscopic Microfracture – the surgeon will clear away the damaged cartilage, and then use a blunt tool to poke a few tiny holes in the bone under the cartilage. Like abrasion arthroplasty this procedure is used to get the layer of bone under the cartilage to produce a healing response, triggering the formation of new cartilage (mainly fibrocartilage) inside the lesion.
– Shoulder Joint Replacement (or shoulder arthroplasty): the artificial joint or prosthesis is made up of 2 parts – a humeral component (a metal hemisphere which is attached to a metal stem) which replaces the round humeral head, and a glenoid component which replaces the glenoid socket. The glenoid component has a flat metal plate that attaches directly to the bone, and a cup-shaped plastic socket. Depending on the extent of the arthritis, it may be necessary only to replace the humeral head, in which case, the patient’s glenoid is left intact and only the humeral component is used.
Your surgeon will make an incision on the front of your shoulder, and after moving aside the muscles he will cut into the joint capsule. Then he will remove the damaged bone from the head of the humerus and make a hole down into the bone, into which the metal stem of the humeral component will be inserted. Next he will prepare the glenoid, removing any remaining cartilage from the surface, and making holes in the bone for anchoring the glenoid component of the prosthesis. Finally the 2 components are inserted into the prepared holes and pressed into place (uncemented prosthesis), or they may be fixed with special cement (cemented prosthesis). Once the new joint is in place, the surgeon will check the correct functioning of the joint, and then he will stitch up the joint capsule. The muscles are then returned to their normal position and the incision is closed with stitches.
AC joint arthritis
– Arthroscopic Resection Arthroplasty: firstly, your surgeon will make two 4-5mm incisions in your shoulder. Through one he will insert a fibre-optic camera to look into the joint, and through the other, he will pass the surgical instruments. He will remove a small piece of bone from the end of the clavicle (less than 1cm), taking care not to damage the ligaments that link the acromion and the clavicle together. As your body heals after the operation, the bone removed will be replaced by scar tissue. The surgeon will also remove any bone spurs or inflamed tissue.
Rehabilitation after surgery
Arthroscopic debridement: you should wear a sling for the first few days after the operation to rest your shoulder, and you will be given physiotherapy exercises to rebuild your muscles and restore a full range of movement.
Bone marrow stimulation procedures: you will wear a sling for about 6 weeks after the operation. You will start passive physiotherapy exercises immediately after the operation and then move on to active strengthening and range of motion exercises after about 4-6 weeks. The physiotherapy programme will last 3-4 months.
Shoulder joint replacement: you will have to wear a sling for about 6 weeks after the operation, and you may be given ice-packs or electrical stimulation to ease your joint. Physiotherapy will begin immediately with the first treatments aimed at reducing pain and swelling, and then you will move on to passive stretching and range of motion exercises – ie your therapist will move your arm for you. After 3 weeks, you can start active shoulder exercises to regain your range of movement and rebuild your muscles, and you will continue this programme for 3-4 months.
Arthroscopic resection arthroplasty: you will wear a sling to support your shoulder for 1-2 weeks after the operation, and you may be given ice-packs or electrical stimulation treatments to help ease the shoulder. Physiotherapy will start straight away, with the first treatments aimed at reducing pain and swelling, and then you will start light stretching and range of motion exercises. After a couple of weeks the exercises will become more strenuous in order to build up the rotator cuff muscles and to ensure perfect co-ordination during movement.
When will I be back to normal?
Arthroscopic debridement – depending on the type of work you do, you should be able to resume work between 2-7 days after the operation, and driving after a week. Normal sporting activity can be resumed after 2 weeks.
Bone marrow stimulation procedures – office work and driving can be resumed after 10-15 days, manual work after 30-45 days. You should be able to return to light sporting activity after 2 months, and contact sports after 6 months.
Shoulder joint replacement – office workers can go back to work 15-20 days after the operation, although manual workers should wait 45-60 days, depending on the kind of arm movements their work requires. You can start light sporting activity after 2 months, and contact sports after 6 months.
Arthroscopic resection arthroplasty – you can return to office work and driving after about a week, although manual workers may need to wait 4-6 weeks before resuming work, depending on the kind arm movements required. After 6 weeks you can return to normal sporting activity.